
Medication non‑adherence remains one of health care’s most persistent and expensive challenges.
Across chronic conditions, only about half of patients take medications as prescribed, even when effective treatments are available. The consequences are significant: disease progression, avoidable hospitalizations, increased mortality, and hundreds of billions of dollars in preventable health care costs each year.
Health systems aren’t blind to the problem. In many cases, they can already predict it. But prediction alone isn’t enough. Risk scores sitting in dashboards don’t change outcomes unless they are translated into timely, personalized action.
This is where agentic AI and the ability to operationalize analytics at scale become transformative.
Seeing the risk isn’t the same as acting on it
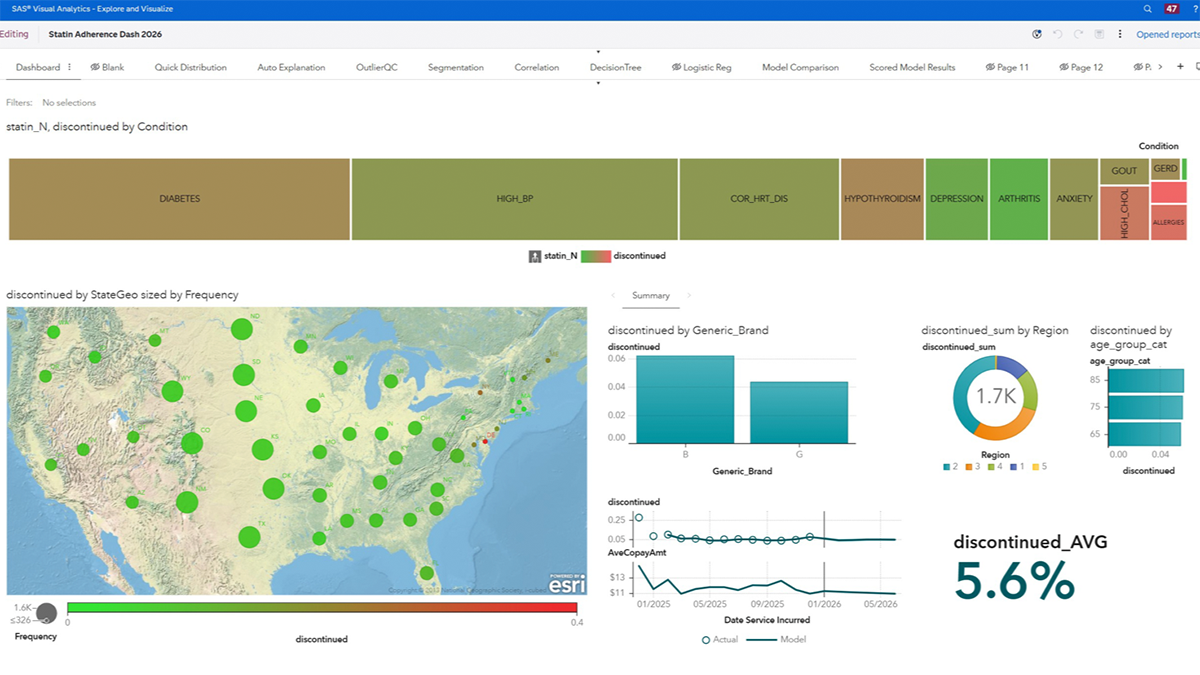
Combining historical claims and clinical data to identify at-risk patients is now table stakes. Dashboards highlight key performance indicators, geographic patterns and outliers, creating shared awareness across clinical, operational and analytics teams.
But it’s only the first step. What matters most is confidence in the models driving these insights.
Trustworthy models are what make action possible
Before any intervention happens, there’s a more basic question: should you trust the signal?
Behind every risk score is a set of models competing to explain patient behavior. Different methodologies – proprietary, open source, statistical and machine learning – are tested to determine the best performer. For organizations using SAS® Model Manager, the solution governs this entire life cycle, enabling champion‑challenger comparison, versioning, monitoring and traceability.
Then there’s SAS model scorecards, often described as “nutrition labels for analytics”. The model scorecards communicate purpose, performance, fairness and limitations, giving stakeholders confidence that models are production‑ready and appropriate for real clinical decisions.
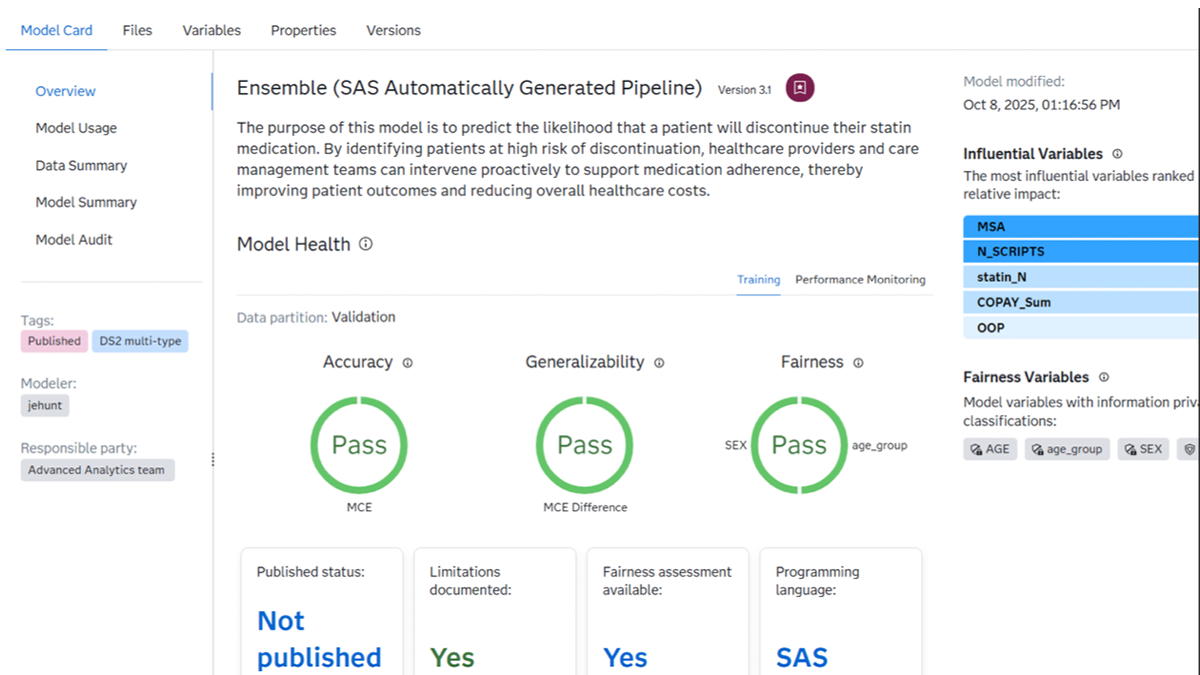
Teams need to understand what a model is doing, where it may fall short and whether it is appropriate. Without that foundation, risk scores don’t drive action; they only prompt hesitation.
From score to decision
Once risk is established, the real work begins: deciding what to do about it.
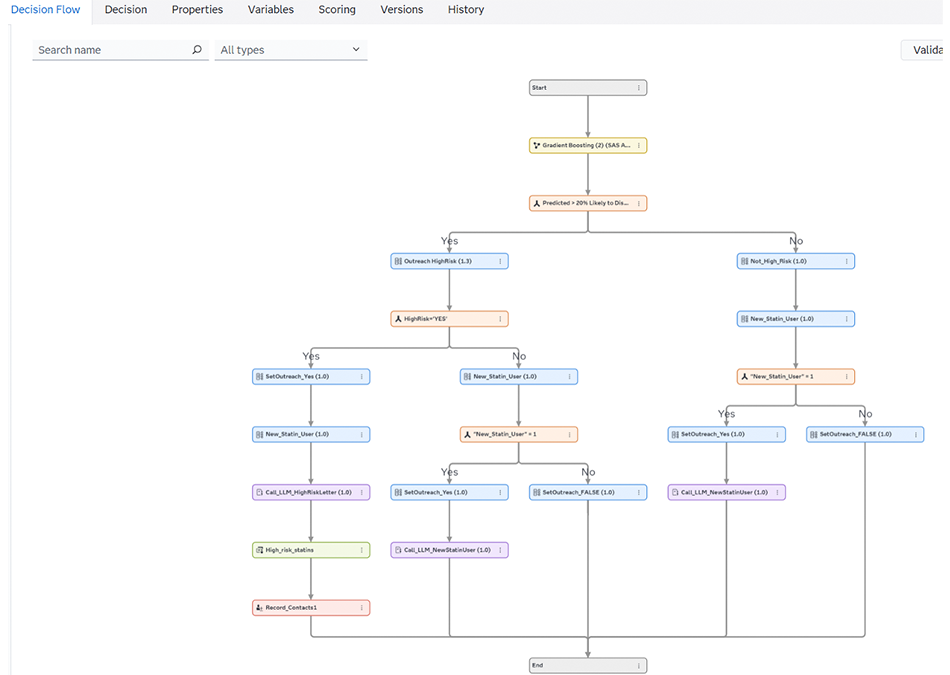
Not every patient needs the same response. Some require no outreach. Others need monitoring. A smaller group needs timely, targeted intervention. The challenge is consistently translating a prediction into the right next step. That requires decision logic.
By combining rules with model outputs, organizations can route patients along different paths based on the specific actions needed, not broad assumptions. The result is a system that prioritizes attention where it matters most, rather than spreading effort evenly and hoping for impact
Decisioning in practice: Platforms like SAS® Intelligent Decisioning connect model output directly to next-best actions
Agentic AI in action
The moment of action is where things often break down. Even when high‑risk patients are identified, outreach is frequently generic, delayed or inconsistent. Personalization doesn’t scale easily when care teams are already stretched. This is where agentic AI becomes practical.
With a defined decision flow, an AI agent can generate personalized, clinically appropriate outreach. The agent configured for patient‑specific context – such as medication history and discontinuation risk – generates tailored messages that encourage adherence, acknowledge progress and prompt patients to engage with their care team.
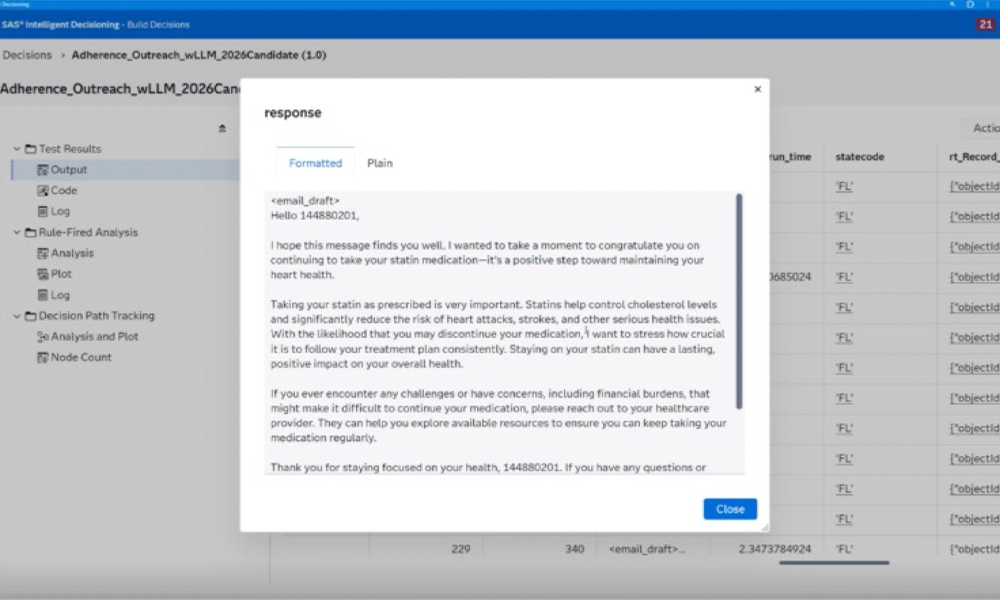
Just as important are clearly defined guardrails. Tone, content, urgency and escalation logic are all explicitly controlled, enabling human‑in‑the‑loop or human‑on‑the‑loop oversight. The result is scalable personalization without sacrificing trust, safety, or governance.
Turning insight into impact
Medication adherence is one example of a broader pattern.
Across health care, organizations struggle to act on insights in a timely manner.
The same approach extends naturally to other high‑impact clinical workflows. Predictive models can identify patients at risk during transitions of care, flagging individuals who may require additional follow‑up after discharge to prevent readmissions or care gaps.
Decisioning frameworks can also support the construction of concise clinical summaries for nurse‑to‑nurse hand‑offs, synthesizing key patient data, recent interventions and risk flags to improve continuity and reduce cognitive burden during shift changes. Analytics and agentic AI can also assess the likelihood of antibiotic prescribing behaviors, helping stewardship teams identify patterns that deviate from evidence‑based guidelines and proactively intervene with targeted education or decision support.
In each case, the same foundation applies: trusted models, transparent governance and intelligent workflows that ensure insights are delivered at the right moment, to the right person, in a form that supports safer, more effective care.
By connecting trusted analytics to action, organizations can move beyond identifying risk to actually reducing it – improving patient outcomes, reducing avoidable costs and operationalizing AI responsibly at scale.
