The creation of Health Information Exchanges (HIEs) took off in 2009 with the establishment of the State Health Information Exchange Cooperative Agreement Program (SHIECAP). Recently, it seems like HIEs have been somewhat of the middle-child, garnering less attention between the health insurance exchanges and Medicaid expansion. But let’s take a look at where HIEs are headed in 2013, and beyond.
To-date, most of the efforts surrounding HIE have been focused on connectivity, interoperability, and supporting Meaningful Use. Challenges surrounding the financing and sustainability of HIEs have also been top-of-mind for both private and public HIEs. While private HIEs have been considered more promising in terms of sustainability, it appears that public HIEs also have a positive future. In fact, 37 state-designated HIEs recently indicated that they fully expect to be operational three years from now, after SHIECAP ends, and assuming no further funding. This indicates a great deal of confidence that they can continue operations even without federal dollars[1].
Even better is that 88 advanced HIEs – more than ever -- were identified in 2012, several of which are statewide HIEs, such as the Kentucky Health Information Exchange, ConnectVirginia, and the Michigan Health Information Network. Advanced HIEs are those that have reached stage 5, 6, or 7 on the eHealth Initiative’s HIE development scale. As more HIEs approach these advanced stages, what’s next on the radar? What types of activities should be occurring in Level 7 – the Innovating stage?
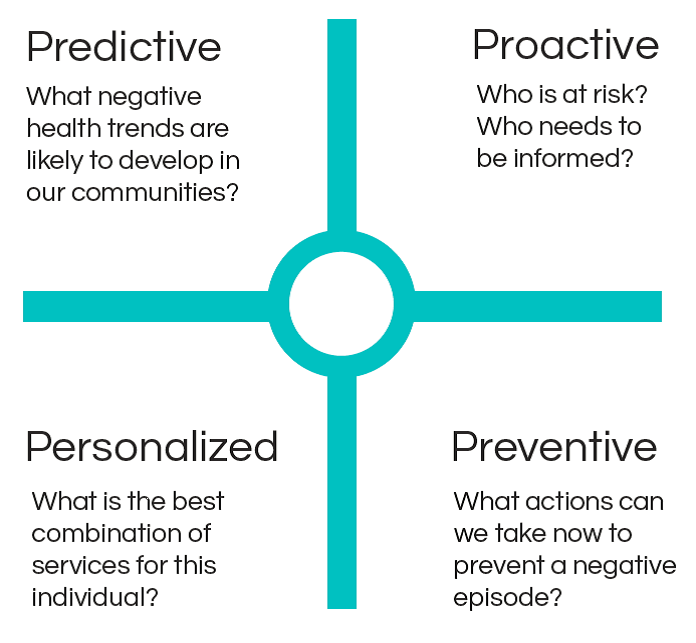
The union of HIE and analytics is the inevitable next step on the path of HIE innovation. Analytics allow clinical data to be mined and translated into actionable information to track and measure outcomes, identify gaps in service, and even forecast individual trajectories of health. Essentially, analytics can give providers a 360-degree view of their patients that will help achieve the 4 P’s of quality in our healthcare system.
HIEs create a clinical data repository (CDR) that consolidates data from a variety of clinical sources like clinical summaries, physician notes, medication lists, labs, vital statistics, and referrals; data elements that medical claims do not provide. For example, let’s say John went to his primary care physician for an annual check-up. The claim would simply inform us that John did have his annual physical, which is certainly good information (and good news), but it would not tell us, for instance, that John was diagnosed with high blood pressure, that his sugar levels are rising, or other indicators that are essential in treating John holistically.
This information is critical to all providers that care for John, and especially essential for value-based payment models. As accountable care organizations (ACOs) and patient-centered medical homes (PCMHs) continue to emerge, they will rely heavily upon ’big analytics’ to succeed, making HIE analytics even more essential. A recent report by Frost & Sullivan stated:
"Participants in HIE will continue to gravitate towards organizations and technology vendors capable of providing a wide range of solutions and services, particularly value-added services that enable patient engagement and predictive analytics needed to better manage patient populations and contain risk, especially for emerging accountable care organizations (ACOs).” [2]
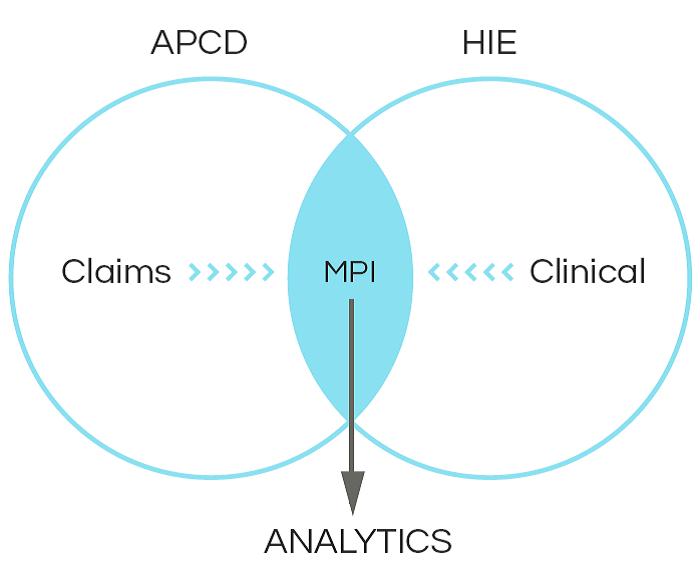
While claims data alone cannot give us details into John’s health, it certainly can enhance clinical information by allowing us to understand the costs associated with treating him. As I mentioned in my 4 P’s blog post, linking HIE with other datasets, like an all-payer claims database, can help us understand costs, quality, and outcomes. Though these linkages will require overcoming technical and legal issues, such as the creation of a Master Patient Index (MPI), it is a potentially great merger. Perhaps John has several claims for specialty doctors over the course of the months and even an ER visit. Leveraging clinical data would help us to understand what happened that led up to these events. Maybe there was a medication that should (or should not) have been prescribed, or a missed preventive procedure. Moreover, the linkage of these datasets lets us be proactive in helping prevent negative episodes in John’s future.
States like Maine are already getting started on these efforts, and others like Kansas are connecting their HIEs to national disease outbreak surveillance data, like that of CDC BioSense. There’s no doubt that analytics are going to be valuable and necessary for HIEs. I’m excited to see what innovations public HIEs bring in 2013. Happy New Year!
[1] http://www.ehealthinitiative.org/resources/viewdownload/54-annual-surveys/613-2012-report-on-health-information-exchange-supporting-healthcare-reform.html
[2] http://www.frost.com/c/10057/sublib/display-report.do?id=N8A7-01-00-00-00

{kind=link}